System Factors in Patient Safety
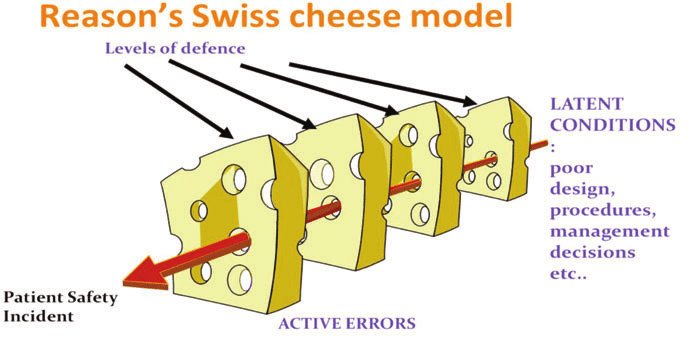
James Reason created the Swiss cheese model to explain how faults in different layers of a system lead to incidents. This model shows how a fault in one layer of a health care system of care is usually not enough to cause an accident. Adverse events usually occur when a number of faults occur in a number of layers (for example, fatigued workers plus inadequate procedures plus faulty equipment) and momentarily line up to permit a “trajectory” of accident opportunity.
Lets see the scenario of a medication error happening in a patient as an example:
He was having heartburn for quite a few days. Not able to take it much longer, Madhav visited the doctor. He explained his symptoms and the doctor wrote a simple prescription for heartburn but the writing was not clear.
Madhav did not clarify the medication name with the physician and took the prescription to the pharmacist.
The pharmacist deciphered the medication to the best of his understanding and dispensed the medication.
Madhav returned two days later with completely different symptoms in addition to continuing heartburn, a review revealed that the patient was dispensed aripiprazole, an antipsychotic instead of rabeprazole, an anti ulcer drug, and the symptoms the patient was experiencing now were the adverse reactions of the incorrect drug he was taking.
Now, who is at fault here, there were many barriers to this medication error – the doctor (if he gave computerized prescription or made sure the hand writing was clear), Patient (who could have confirmed the medication name with the physician), the pharmacist (who understood the concept of a sound alike drugs and made sure to confirm it with the physician). All the barriers missed the check points and the the holes of the swiss cheese model aligned for this error to happen.
Looking at it from systems approach, there are various factors involved – the issue of illegible hand written prescription, the lack of training of the pharmacist on sound alike drugs. Awareness at patient level.
So, when we go to the root of it, there is a need to review systems in healthcare that are error prone and change them. The first step towards doing root cause analysis is reporting errors. The major road block to reporting is the culture of blame and shame of an individual, which discourages individuals from reporting AEs or errors.
The National patient safety implementation framework calls for establishing an error and AE reporting system that is non-punitive, confidential, independent, timely, system oriented and responsive in nature.
The change is coming
#PhVFITpatientsafetycampaign