I have been a big fan. Not only for the amazing Dr. Gregory House, and the story line but because this series gives you a glimpse of the struggles, challenges and beauty of medical profession. And also, the series educates on so many relevant healthcare topics.
Why I talk about it today during our patient safety campaign? Because it was about 12 years ago when I first saw the Dr. House episode on “hospital-acquired infections” (HAI) with a mention on “antibiotic resistance”.
It is a very powerful story they tell, which has stayed with me for years. This episode not only educates you about the problem but also how due diligence and vigilance towards HAI saved from an epidemic in the hospital.
If you would like to watch it, do watch “Maternity”, episode 4, Season 1, Dr. House. Its available on Prime.
It will help bring some perspective if you are a non medic and would like to understand the patient safety topic “Hospital acquired infections” which is the Goal 5 given by NABH.
See an excerpt from the Maternity episode under the youtube link above
If you are working on oncology studies, have you noticed that complete radical mastectomy is usually reported pre-1980 for breast cancer patients. Have you thought about the reason?
Radical mastectomy used to be a norm in America after Halsted first established the procedure in 1894. This Surgery entailed removal of breast, chest muscles, and all of the lymph nodes under the arm, and this was thought to be the only option to treat breast cancer. Halsted based his surgery on centrifugal theory. In Emperor of all maladies, Siddhartha Mukherjee explains this as – cancer like a malevolent pinwheel, tended to spread in ever-growing arcs from a single central focus in the body. A surgeon’s job was to arrest the centrifugal speed by cutting every piece of it out of the body, as if to catch and break the wheel in midspin. The more a surgeon cut, the more it cured. However, morbidity after the operation was great, because the large wounds were left to heal by granulation, lymphedema was near universal, and arm movement was severely restricted (due to pectoralis muscle removal and damage to axilla nerves). For these reasons, chronic pain was also an important sequela.
Another oncologist Geofferey Keynes was not so convinced about Halsted’s theory. 1n 1924, from experience with his patients, he saw that a lumpectomy, a much less invasive procedure along with radiation, worked just as well but with much less morbidity. The relapse rates were almost equal as with Radical mastectomy but the quality of life for the patients was much better. He presented his data but his ideas were not taken seriously as the surgeons of that time were completely sold to the centrifugal theory.
In 1953 (almost 30 years later), George Crile, a follower of Halsted theory started having his doubts about radical mastectomy. His research and studies revealed that the cancer spread was more erratic and unpredictable. The patients treated with radical mastectomy also relapsed and died due to metastasis. He came to understand that either the breast cancer is a highly localised disease – thus curable by a smaller mastectomy – or an inherently systemic disease – thus uncurable event by the most exhaustive surgery. He gave up radical mastectomy altogether and started following the Keynes’s procedure and saw that the survival rate of patients in the two surgeries had no difference. Separated by 40 years of clinical practice, both Keynes and Crile had seemingly stumbled on the same clinical truth.
However, it took another twenty years, and dedicated efforts and clinical trials by another great oncologist Bernard Fisher to establish the futility and danger of a complete radical mastectomy. It will also be interesting to note that the withdrawal of radical mastectomy was also sped up due to the thalidomide disaster in 1960s. Fallibilities in the medical discipline surfaced and patients recognized that one of the most common and disfiguring operations was never tested in a trial, women refused radical mastectomies. Clinical trials were conducted by Fisher to prove his findings! However, they were not without obstacles. It took him around 10 years to gather all data.
Meanwhile, more mutilating and invasive procedures liked extended radical mastectomy were also tried and abandoned due to high mortality rates!
A radical mastectomy is rarely performed now and has been replaced by less invasive procedures. I wonder if medical fraternity at that time was more accepting of the new ideas and theories, would it have taken as much as almost a century to reach this decision?
Effective #pharmacovigilance is only possible when we have data to assess and analyse.
Are we reporting, are HCPs reporting? I spoke to a friend whose whole family was vaccinated (Covishield), most in the family experienced high fever, severe body pain, injection site pain and swelling. Expected reactions, listed in the Serum Institute of India fact sheet. Lot of people under the age of 50 are experiencing these (atleast 10 cases that I heard).
Another reaction that one of his family members complained of was “Chest pain” for 2-3 days. This is not an expected reaction as per the SII fact sheet or product insert. I asked him if he had reported the reactions anywhere? He was confused – where and who to report?
So, I reported the reactions to SII and PvPI in an email, I received a response from SII with a vaccine AE reporting form to fill for further details on the drug and reactions. I made sure to fill as much details as possible (have been at the other end and know the frustration of having insufficient information).
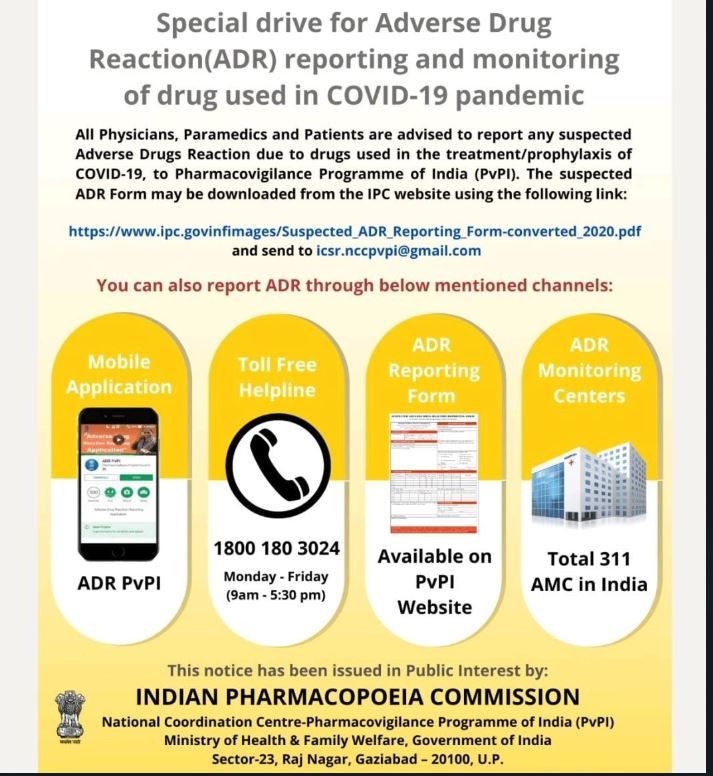
Do you know when and where to report after the #covid19vaccine vaccination? If you don’t, here are some details:
The first person to report is your treating physician who should be reporting the AEs further.
Other ways to report see link below, and PvPI reporting information in the pic attached. You can also report on the helpline numbers provided at Cowin portal in the FAQs document for vaccination.
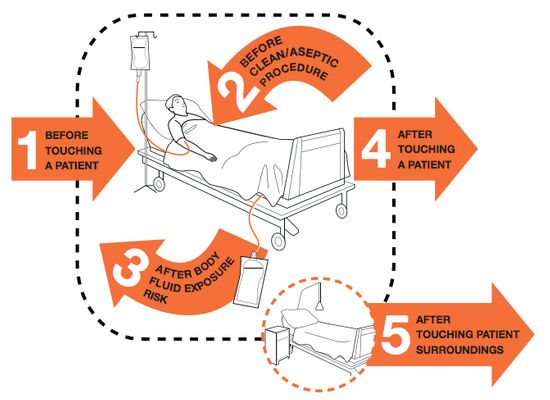
Indian Medical association (IMA) and WHO prescribes 5 Moments for Hand Hygiene for healthcare workers to prevent Hospital acquired infections:
IMA recommends health-care workers to clean their hands:
1. Before touching a patient 2. Before clean/aseptic procedures 3. After body fluid exposure/risk 4. After touching a patient, and 5. After touching patient surroundings
Hand hygiene is one of the simplest ways to avoid HAIs, it is however, often unconsciously missed/ ignored during the day to day working in hospitals.
How can patients help with this?
Simple awareness about these hand hygiene practices can make a big difference. Patients and attendants can remind the health care workers caring for the patients regarding these simple hand hygiene practices.
Patient safety needs concerted efforts from all stake holders, physicians, health care workers, patients, and care takers alike. Are you ready to take the lead?