A PhVFit initiative where we bring to you insights on patient safety from industry and healthcare experts. The insights are conversation starters and food for thought, a joining of hands for a movement in patient safety.
This Month, we have Dr. Maya Sharma, Global Medical Director, Modi Mundipharma & Win Medicare, sharing her thoughts with us.
Thank you Dr. Maya for sharing your valuable insights with us!
A robust reporting system is the foundation of any pharmacovigilance system, there is a dire need of strengthening the reporting system in India to make Pharmacovigilance an active practice to ensure patient safety. Robust PV systems and PV training across all stakeholders is need of the hour!
What is the probability of a house catching fire? Very bleak, right.
In the society where my parents live, the lane surrounding the building is narrow. Due to the lack of ample parking area, the extra cars are parked on the lane, which leaves not much space. There was a talk from RWA some time ago on building sheds for that parking space so that people get the covered parking (something builder had promised).
Elders from the society started resisting that move giving the reason that it will become a permanent structure and no big vehicle (e.g. a fire brigade) can then be brought in easily – in case of a fire incident. The team insisting on building sheds did not seem to get the point, whats the probability of a house catching fire, right??
However, the elders kept their foot down and even filed a case to stop this from happening. The project was stalled.
And then it happened! The flat diagonally opposite ours (on the same floor) caught fire. It was an accident and in a matter of half an hour, the fire reached the flats above. The fire extinguishers installed in the society were faulty and were not working. The fire brigade was called. It took some time to remove the cars from there, so that a fire brigade vehicle can enter. It took hours extinguishing the fire and the house was devastated.
Now, imagine, had they built the sheds, how fire brigade would have entered! Yes, fire incidents happen rarely but does that mean we do not plan for them? Risk management, assessment and mitigation is a very important part of any process.
Why am I telling you this story?
The main purpose of pharmacovigilance is also risk mitigation and management. The possibility of an Adverse event happening might be 1 in a million, but the data we collect and assess gives us an understanding on how to manage that risk. Clotting events with vaccines is a rare event, but if a patient unfortunately experiences it, the knowledge can help in early diagnosis and management of the event (when we know the cause) and can save lives! This is the reason, we need a robust reporting and analytics system in Pharmacovigilance, so that risks can be assessed and mitigated.
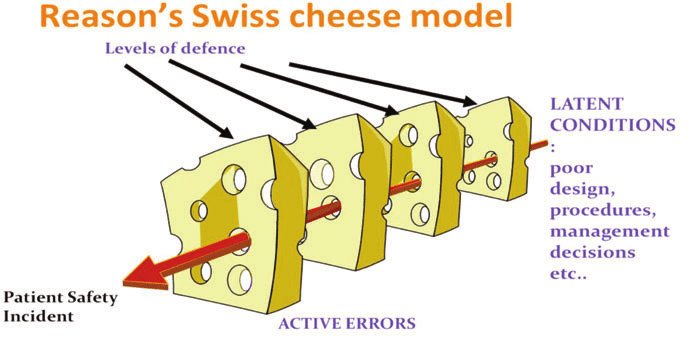
James Reason created the Swiss cheese model to explain how faults in different layers of a system lead to incidents. This model shows how a fault in one layer of a health care system of care is usually not enough to cause an accident. Adverse events usually occur when a number of faults occur in a number of layers (for example, fatigued workers plus inadequate procedures plus faulty equipment) and momentarily line up to permit a “trajectory” of accident opportunity.
Lets see the scenario of a medication error happening in a patient as an example:
He was having heartburn for quite a few days. Not able to take it much longer, Madhav visited the doctor. He explained his symptoms and the doctor wrote a simple prescription for heartburn but the writing was not clear. Madhav did not clarify the medication name with the physician and took the prescription to the pharmacist. The pharmacist deciphered the medication to the best of his understanding and dispensed the medication.
Madhav returned two days later with completely different symptoms in addition to continuing heartburn, a review revealed that the patient was dispensed aripiprazole, an antipsychotic instead of rabeprazole, an anti ulcer drug, and the symptoms the patient was experiencing now were the adverse reactions of the incorrect drug he was taking.
Now, who is at fault here, there were many barriers to this medication error – the doctor (if he gave computerized prescription or made sure the hand writing was clear), Patient (who could have confirmed the medication name with the physician), the pharmacist (who understood the concept of a sound alike drugs and made sure to confirm it with the physician). All the barriers missed the check points and the the holes of the swiss cheese model aligned for this error to happen.
Looking at it from systems approach, there are various factors involved – the issue of illegible hand written prescription, the lack of training of the pharmacist on sound alike drugs. Awareness at patient level. So, when we go to the root of it, there is a need to review systems in healthcare that are error prone and change them. The first step towards doing root cause analysis is reporting errors. The major road block to reporting is the culture of blame and shame of an individual, which discourages individuals from reporting AEs or errors.
The National patient safety implementation framework calls for establishing an error and AE reporting system that is non-punitive, confidential, independent, timely, system oriented and responsive in nature. The change is coming
To err is human, and this is why it is so important to apply human factors for patient safety, and develop procedures to minimize error.
How we apply human factors? Aviation industry applies the principles of human factors, and has built a controlled system of checklists and protocols to minimize the errors! The stakes are so high, you can not afford to err in avaiation, right.
Now just imagine how all the more important human factors are in a hospital environment. However, research has shown that human factors and ergonomics are often ignored in health care.
In a health care environment, there are a number of human factors involved that can lead to errors. To name a few, fatigue due to longer shifts, stress of emergencies, change of duties that can lead to communication issues during handovers, distractions during procedures, etc.
For e.g. a lab technician takes samples for a patient in a common ward, and soon after is called by another patient for some support, however, in the hurry, he misses labeling the samples and they get mixed up. If we understand this common human factor, it makes sense to develop a protocol to minimize the distractions.
Time outs in operation theatre before starting an operation is also an example of a protocol to minimize procedural errors.
The problem starts when the protocols are deviated from, example the surgeon feels he knows all details and does not need a time out.
Therefore, the protocols are not enough, adherence to them is most essential. A failure to apply human-factors principles is a key aspect of most adverse events (harm to patients) in health care.
The WHO’s curriculum guide for patient safety recommends: all health-care workers to have a basic understanding and training of human-factors principles, and according to this understanding the ergonomics of the health care facility should be customized to minimize error.
Let us take another example:
Here is an insightful article from Uppsala Monitoring Centre Uppsala reports that talks about the medication errors due to two component vaccines and the harm they could cause (link at the bottom).
What kind of errors?
The article shares a number of real life medication error examples that have happened in different countries across the world – and their impact. Errors like:
The vaccine components do not mix properly or incorrect diluent was used to reconstitute a vaccine.
The Impact:
In 2014, 15 children in Syria died after atracurium (a paralysing agent) was used to reconstitute a measles vaccine. Apparently the ampule packaging of the drug was similar to the vaccine diluent packing and the mix-up occurred.
A similar incident in Samoa in 2018 not only led to the death of two infants but also impeded the immunisation efforts in the country, which in turn led to an outbreak of measles in the country that infected 4300 people and claimed 70 lives (majorly 5 year olds).
These were common human errors, but when you go the root of it, you find they could have been prevented.
The article further states, “human error can never be eliminated, however, many factors that contribute to the error can be identified and improved to minimize the chances of it occurring. International medication safety network (IMSN) has issued a position statement calling for greater worldwide attention to the problem of unsafe design of vaccine packaging and labeling”.
To err is human, but not to learn from errors and keep erring is not!
Read further under the link below. It is a must read, do not miss.
Incident that laid the foundation of Pharmacovigilance
In 1957, a drug was marketed as a safe sedative by a German company. They advertised their product as “completely safe” for everyone, including mother and child, “even during pregnancy,” as its developers “could not find a dose high enough to kill a rat.” By 1960, it was marketed in 46 countries, with sales nearly matching those of aspirin.
Around this time, Australian obstetrician Dr. William McBride discovered that the drug also alleviated morning sickness. He started recommending this OFF-LABEL use of the drug to his pregnant patients, setting a worldwide trend.
In 1961, a lot of reports about birth defects started coming in from all over the world. As Dr. McBride dug deeper, he began to associate this so-called harmless drug with severe birth defects in the babies he delivered. The drug interfered with the babies’ normal development, causing many of them to be born with phocomelia, resulting in shortened, absent, or flipper-like limbs.
What followed was the biggest man‐made medical disaster ever, where numberless miscarriages happened and over 10,000 children were born with a range of severe and debilitating malformations. . Can you guess the drug?
Yes, the drug is thalidomide. A drug that caused the biggest man-made disaster where more than 10,000 children were born with deformities all over the world.
But do you know the tragedy was largely averted in United States – thanks to FDA inspector Frances Kelsey, who prevented the drug’s approval within the United States despite pressure from the pharmaceutical company and FDA?
-The application for thalidomide contained incomplete and insufficient data on its safety and effectiveness. -The lack of data indicating whether the drug could cross the placenta, which provides nourishment to a developing fetus. -There were not yet any results available from U.S. clinical trials of the drug. Even if these data were available, they may not have been entirely reliable as then clinical trials did not require FDA approval. The trial in US involved distribution of 2.5 m tablets to 20000 patients but the results and AEs were not tracked by physicians.
Due to her stand, the tragedy was largely averted, and she subsequently was given a distinguished service award by President JFK.
The tragedy and crisis laid the foundation of present-day Pharmacovigilance.
Thalidomide was banned in most countries by March 1962.
The book “The power of habit” talks about the “power of crisis”:
Great leaders make crisis in a business/ process an opportunity for bringing in transformational changes in the organization.
The crisis in drug safety led to strict legislations- that immediately followed the Thalidomide disaster and laid the foundation of PV:
– The whole regulatory system was re-shaped in the UK where a Committee on the Safety of Drugs (CSD) was started in 1963 followed by a voluntary adverse drug reaction reporting system(Yellow Card Scheme) in 1964.
– In the United States, the Drug Amendments Act of 1962 was passed by Congress requiring the FDA to approve all new drug applications (NDA) and, for the first time, demanded that a new drug should be proven to be effective and safe. Of equal importance, the FDA was also given the authority to require compliance with current Good Manufacturing Practices (GMP), to officially register drug establishments and implement other requirements. The EEC Directive 65/65/EEC on the approximation of provisions laid down by law, regulation and administrative action relating to medicinal products was also induced by the thalidomide disaster.
In 1965, Thalidomide was re-marketed in several countries for erythema nodosum leprosum (ENL) and cases of thalidomide deformities have re-emerged.
This is specially in Brazil where leprosy cases are maximum, and the drug is used widely.
Schuler-Faccini and other researchers from the Universidade Federal do Rio Grande do Sul in Porto Alegre looked at the birth records of 17.5 million babies born between 2005 and 2010. They looked at all children with limb defects and those with the characteristic defects of Thalidomide and compared the distribution of Thalidomide tablet with the number of limb defects and found a direct correlation.
“The bigger the amount of pills in each state the higher the number of limb defects.”
In the same 2005-2010 period, 5.8 million Thalidomide pills were distributed across Brazil and about 100 known cases were reported in these six years similar to Thalidomide syndrome.
Several thalidomide babies continue to be born each year!
Between 2015 and 2018, 5 new cases of use of thalidomide during pregnancies were reported to the Mohr and ANVISA. Reason?
Regulatory insufficiency, self-medication, and widespread use under inadequate supervision.
I have been a big fan. Not only for the amazing Dr. Gregory House, and the story line but because this series gives you a glimpse of the struggles, challenges and beauty of medical profession. And also, the series educates on so many relevant healthcare topics.
Why I talk about it today during our patient safety campaign? Because it was about 12 years ago when I first saw the Dr. House episode on “hospital-acquired infections” (HAI) with a mention on “antibiotic resistance”.
It is a very powerful story they tell, which has stayed with me for years. This episode not only educates you about the problem but also how due diligence and vigilance towards HAI saved from an epidemic in the hospital.
If you would like to watch it, do watch “Maternity”, episode 4, Season 1, Dr. House. Its available on Prime.
It will help bring some perspective if you are a non medic and would like to understand the patient safety topic “Hospital acquired infections” which is the Goal 5 given by NABH.
See an excerpt from the Maternity episode under the youtube link above
If you are working on oncology studies, have you noticed that complete radical mastectomy is usually reported pre-1980 for breast cancer patients. Have you thought about the reason?
Radical mastectomy used to be a norm in America after Halsted first established the procedure in 1894. This Surgery entailed removal of breast, chest muscles, and all of the lymph nodes under the arm, and this was thought to be the only option to treat breast cancer. Halsted based his surgery on centrifugal theory. In Emperor of all maladies, Siddhartha Mukherjee explains this as – cancer like a malevolent pinwheel, tended to spread in ever-growing arcs from a single central focus in the body. A surgeon’s job was to arrest the centrifugal speed by cutting every piece of it out of the body, as if to catch and break the wheel in midspin. The more a surgeon cut, the more it cured. However, morbidity after the operation was great, because the large wounds were left to heal by granulation, lymphedema was near universal, and arm movement was severely restricted (due to pectoralis muscle removal and damage to axilla nerves). For these reasons, chronic pain was also an important sequela.
Another oncologist Geofferey Keynes was not so convinced about Halsted’s theory. 1n 1924, from experience with his patients, he saw that a lumpectomy, a much less invasive procedure along with radiation, worked just as well but with much less morbidity. The relapse rates were almost equal as with Radical mastectomy but the quality of life for the patients was much better. He presented his data but his ideas were not taken seriously as the surgeons of that time were completely sold to the centrifugal theory.
In 1953 (almost 30 years later), George Crile, a follower of Halsted theory started having his doubts about radical mastectomy. His research and studies revealed that the cancer spread was more erratic and unpredictable. The patients treated with radical mastectomy also relapsed and died due to metastasis. He came to understand that either the breast cancer is a highly localised disease – thus curable by a smaller mastectomy – or an inherently systemic disease – thus uncurable event by the most exhaustive surgery. He gave up radical mastectomy altogether and started following the Keynes’s procedure and saw that the survival rate of patients in the two surgeries had no difference. Separated by 40 years of clinical practice, both Keynes and Crile had seemingly stumbled on the same clinical truth.
However, it took another twenty years, and dedicated efforts and clinical trials by another great oncologist Bernard Fisher to establish the futility and danger of a complete radical mastectomy. It will also be interesting to note that the withdrawal of radical mastectomy was also sped up due to the thalidomide disaster in 1960s. Fallibilities in the medical discipline surfaced and patients recognized that one of the most common and disfiguring operations was never tested in a trial, women refused radical mastectomies. Clinical trials were conducted by Fisher to prove his findings! However, they were not without obstacles. It took him around 10 years to gather all data.
Meanwhile, more mutilating and invasive procedures liked extended radical mastectomy were also tried and abandoned due to high mortality rates!
A radical mastectomy is rarely performed now and has been replaced by less invasive procedures. I wonder if medical fraternity at that time was more accepting of the new ideas and theories, would it have taken as much as almost a century to reach this decision?
Effective #pharmacovigilance is only possible when we have data to assess and analyse.
Are we reporting, are HCPs reporting? I spoke to a friend whose whole family was vaccinated (Covishield), most in the family experienced high fever, severe body pain, injection site pain and swelling. Expected reactions, listed in the Serum Institute of India fact sheet. Lot of people under the age of 50 are experiencing these (atleast 10 cases that I heard).
Another reaction that one of his family members complained of was “Chest pain” for 2-3 days. This is not an expected reaction as per the SII fact sheet or product insert. I asked him if he had reported the reactions anywhere? He was confused – where and who to report?
So, I reported the reactions to SII and PvPI in an email, I received a response from SII with a vaccine AE reporting form to fill for further details on the drug and reactions. I made sure to fill as much details as possible (have been at the other end and know the frustration of having insufficient information).
Do you know when and where to report after the #covid19vaccine vaccination? If you don’t, here are some details:
The first person to report is your treating physician who should be reporting the AEs further.
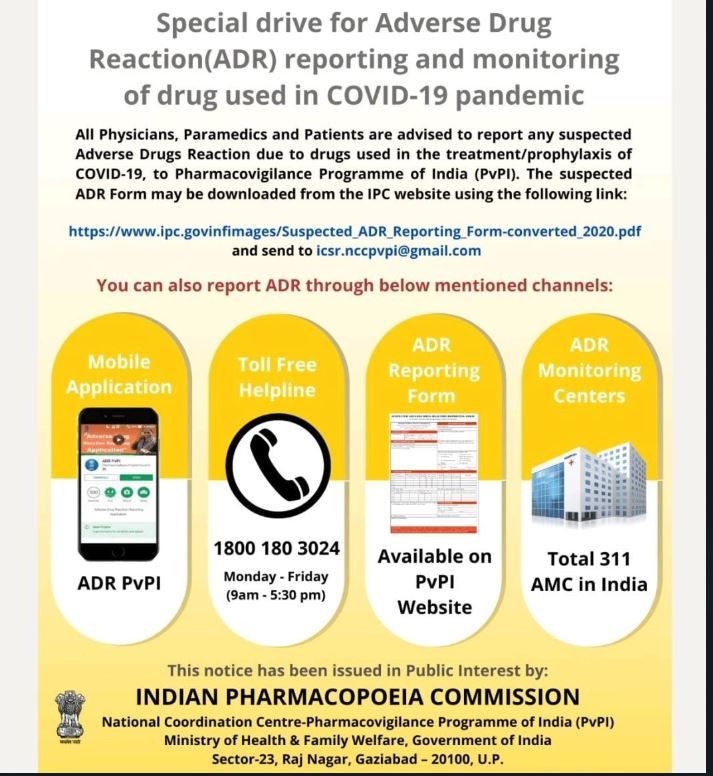
Other ways to report see link below, and PvPI reporting information in the pic attached. You can also report on the helpline numbers provided at Cowin portal in the FAQs document for vaccination.
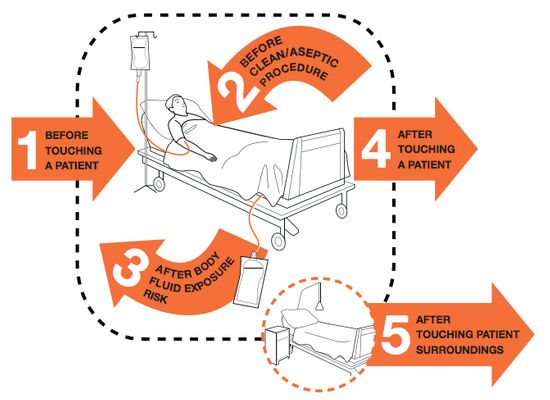
Indian Medical association (IMA) and WHO prescribes 5 Moments for Hand Hygiene for healthcare workers to prevent Hospital acquired infections:
IMA recommends health-care workers to clean their hands:
1. Before touching a patient 2. Before clean/aseptic procedures 3. After body fluid exposure/risk 4. After touching a patient, and 5. After touching patient surroundings
Hand hygiene is one of the simplest ways to avoid HAIs, it is however, often unconsciously missed/ ignored during the day to day working in hospitals.
How can patients help with this?
Simple awareness about these hand hygiene practices can make a big difference. Patients and attendants can remind the health care workers caring for the patients regarding these simple hand hygiene practices.
Patient safety needs concerted efforts from all stake holders, physicians, health care workers, patients, and care takers alike. Are you ready to take the lead?